Recently Health Education England funded me for a two-day course at Henley Business School on Advancing your Change & OD Practice. Their purpose was to support the Knowledge for Healthcare agenda on knowledge mobilisation. My purpose was to understand where we fit in the Trust’s OD agenda. Over the last couple of years we’ve given increasing amounts of support to our OD department and chatting to our head of OD has revealed that we’re both interested in the same kinds of subjects.
OD has a certain fuzziness about it. People rarely train specifically to go into OD and if you ask people what it is, there is a wide range of answers. Few can answer what is the difference between a change manager and an OD specialist. I favour this definition:
OD is a long-range effort to improve an organization’s problem solving and renewal processes… with the assistance of a change agent, or catalyst, and the use of the theory and technology of applied behavioural science, including action research (French & Bell 1999).
The field evolved in 1950’s America, with the work of the National Training Laboratory on group dynamics and leadership (credited for the idea of experiential learning) and the work of Kurt Lewin in the development of T group at the Tavistock Institute, where participants focus more on group dynamics as a way of improving learning and self-awareness. This idea of self-awareness and the concept of ‘use of self’ or ‘self as instrument’ is what defines OD. Dr Mee-Yan Cheung-Judge is the primary author in this area and defines ‘use of self’ as:
Whenever we are in flow with our external observation and awareness, our internal awareness of the “here and now”, and using resources we have (e.g. intellect, cognitive ability, perceptual insights, emotional texture, personality, experience, values, character, skills, social sensitivity, etc.) based on our discerning judgement/intentional choice of decisions as to what right course of action we are willing to put ourselves on the line to execute the work in order to achieve the impact the situation requires.
This is a rather wordy definition, but one which might resonate with those who practice mindfulness or the ‘deep listening’ of coaching. This is where the overlap begins to happen with knowledge mobilisation. In the NHS people are becoming more aware that decisions are not just wholly evidence based, but need to acknowledge the emotional content within. We are seeing more activities such as Schwarz Rounds and Nancy Kline Rounds which support this recognition and check the emotional well-being of the organisation.
When trying to make sense of the organisation and the VACU world (Volatile, Uncertain, Complex and Ambiguous), OD has developed three different schools of thought known as the 3Ds of OD.
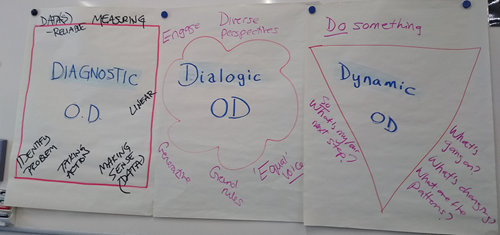
1. Diagnostic OD
This is a chronological approach which is similar in many ways to project management. It defines the problem, studies it, determines the options, implements, and evaluates the effectiveness of actions. Probably the best known form of this in the NHS is the National Staff Survey, where data is collected about issues such as violence and aggression in the workplace, with further analysis and interventions looking at the underlying issues and solutions. Other techniques include Ladder of Inference, Organisational Energy Questionnaire and Star Model.
This is the earliest form of OD, where learning was data driven, change was for people, driven by the OD specialists and based on behavioural science.
2. Dialogic OD
Social movement changed in the 1980’s when the idea arose that change shouldn’t be done to people. We should instead learn through conversations where people are seen as equal partners. Dialogic OD is driven by positive psychology. This is the area in which most Knowledge Mobilisation lies, using techniques such as Knowledge Cafes, Open Space, Appreciative Inquiry, as well as more typical OD functions such as coaching.
This can be overlaid with diagnostic OD for a really powerful intervention. The example we used was Lewin Forcefield Analysis where someone explained an issue and identified the drivers and benefits for changing and the barriers to it. People had to prioritise four of the elements and then there was a discussion about the possible relationships and tensions between them.
3. Dynamic OD
At long last I know that DO OD actually refers to Dynamic OD. This branch of OD evolved from complexity science in the 2000s. It learns from action and advocates change through the use of networks. It is all about activism.
A good way of doing this is by seeing things through different lenses: for Events, Attention, Emotion and Relations. From these lenses we then look for patterns and areas we need to focus on. Other techniques might include Cynefin framework, Theory U and Informal Coalitions.
Good OD is a blend of all three approaches. Without data OD is ungrounded and dangerous, without dialogue it is imposed and without action it is irrelevant.
For me this struck a chord as I could instantly relate it to the NLP Mercedes Model which links thoughts, feelings and behaviour. Within this model you are good two elements, but weak at the third. I can also see parallels in processes I’ve encountered in libraries. I remember being part of the quality group and working on the all-inclusive library survey and later evolving this as part of the Knowledge for Healthcare Value & Impact to the more dialogic impact stories. There are rumblings at looking at how this can be evolved again. Will we be seeing more action research from libraries?
OD can also work on different levels. For OD action to be effective, it should always work across a minimum of three of the levels. The idea behind this is that one level doesn’t provide context, two levels are linear in nature, and three provides triangulation for deeper understanding.
1. Intra-personal
2. Inter-personal
3. Intra-group
4. Inter-group
5. Intra-unit
6. Inter-unit
7. Bounded system
8. System network
9. Total system
So that was Day one of the course. On day two we had to apply the learning by helping a live business client solve some organisational issues. Alas much of this work was confidential and involved personal reflection on the work. It did help me change my thinking. I’ve always thought that libraries support the OD function in the organisation. In reality it jolted memories of things I did at library school. The conversations with experienced OD practitioners made me realise that I am an OD practitioner too. I was really surprised when someone came up to me and said I was their mentor on the CILIP KM Chartership. In the group I was the only one from the Health sector, but the problems we face and solutions developed are all similar. There was much discussion about SharePoint management, health & wellbeing support and pros and cons of communities of practice over dinner.
There are also a few tips I’ve picked up from the course:
Constellation groups - mark a square on the floor and pretend it is a clock face. You can use as an ice breaker e.g. how far have you travelled and ask the group to sort from 12 being closest to 11.59 being furthest away. You can also use to judge experience in a topic (often this will display group relations as well) or for a spicier take, likelihood of project success or trust in a particular individual. This is of course followed up with further conversation.
The use of the word ‘culture’ or ‘culture change’ is a scapegoating phrase. Change to ‘group dynamics’ and you are more likely to succeed in behaviour changes. It makes it much more personal. Words really do matter, so if you find yourself feeling stuck, try re-framing.
Perceived Weirdness Index is a thing. I’m going to have to Google that one.
It’s worth checking out this website, it is full of helpful ideas and activities to improve group interactions:
If you haven’t checked out the KM research leaflets to come out of the Henley Forum you can find them here.
Susan Smith
Senior Librarian
Mid Cheshire Hospitals NHS Foundation Trust
